Case Materials
Case Navigation
Therac-25 Case
General
Teaching Tools
Case Materials
The material on this page is reprinted from N.G. Leveson, & C.S. Turner. "An Investigation of the Therac-25 Accidents." Computer, Vol. 26, No. 7, July 1993, pp. 18-41. Copyright © 1993 Institute of Electrical and Electronics Engineers. This material is posted here with permission of IEEE. Such permission of the IEEE does not in any way imply IEEE endorsement of any of St. Olaf College's products or services. Internal or personal use of this material is permitted. However, permission to reprint/republish this material for advertising or promotional purposes or for creating new collective works for resale or redistribution must be obtained from the IEEE by sending a blank email message to pubs-permissions@ieee.org. By choosing to view this document, you agree to all provisions of the copyright laws protecting it.
The Operator Interface
The Therac-25 operator controls the machine with a DEC VT100 terminal. In the general case, the operator positions the patient on the treatment table, manually sets the treatment field sizes and gantry rotation, and attaches accessories to the machine. Leaving the treatment room, the operator returns to the VT100 console to enter the patient identification, treatment prescription (including mode, energy level, dose, dose rate, and time), field sizing, gantry rotation, and accessory data. The system then compares the manually set values with those entered at the console. If they match, a "verified" message is displayed and treatment is permitted. If they do not match, treatment is not allowed to proceed until the mismatch is corrected. Figure A. shows the screen layout.
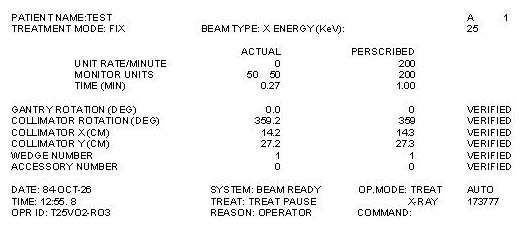
Figure A. Operator interface screen layout
When the system was first built, operators complained that it took too long to enter the treatment plan. In response, the manufacturer modified the software before the first unit was installed so that, instead of reentering the data at the keyboard, operators could use a carriage return to merely copy the treatment site data [Miller]. A quick series of carriage returns would thus complete data entry. This interface modification was to figure in several accidents.
The Therac-25 could shut down in two ways after it detected an error condition. One was a treatment suspend, which required a complete machine reset to restart the machine. If a treatment pause occurred, the operator could press the "P" key to "proceed" and resume treatment quickly and conveniently. The previous treatment parameters remained in effect, and no reset was required. This convenient and simple feature could be invoked a maximum of five times before the machine automatically suspended treatment and required the operator to perform a system reset.
Error messages provided to the operator were cryptic, and some merely consisted of the word "malfunction" followed by a number from 1 to 64 denoting an analog/digital channel number. According to an FDA memorandum written after one accident:
The operator's manual supplied with the machine does not explain nor even address the malfunction codes. The [Maintenance] Manual lists the various malfunction numbers but gives no explanation. The materials provided give no indication that these malfunctions could place a patient at risk.
The program does not advise the operator if a situation exists wherein the ion chambers used to monitor the patient are saturated, thus are beyond the measurement limits of the instrument. This software package does not appear to contain a safety system to prevent parameters being entered and intermixed that would result in excessive radiation being delivered to the patient under treatment.
An operator involved in an overdose accident testified that she had become insensitive to machine malfunctions. Malfunction messages were commonplace — most did not involve patient safety. Service technicians would fix the problems or the hospital physicist would realign the machine and make it operable again. She said, "It was not out of the ordinary for something to stop the machine…It would often give a low dose rate in which you would turn the machine back on…They would give messages of low dose rate, V-tilt, H-tilt, and other things; I can't remember all the reasons it would stop, but there [were] a lot of them." The operator further testified that during instruction she had been taught that there were "so many safety mechanisms" that she understood it was virtually impossible to overdose a patient.
A radiation therapist at another clinic reported an average of 40 dose-rate malfunction, attributed to underdoses, occurred on some days.
Reference: E. Miller, "The Therac-25 Experience," Proc. Conf. State Radiation Control Program Directors, 1987.